2. Chronic Obstructive Pulmonary Disease (COPD)
Chronic obstructive pulmonary disease (COPD) used to describe two conditions—emphysema and chronic bronchitis—that make it difficult to breathe in and out. Today, COPD is simply described as a disease characterized by chronic airflow limitation caused by small airway disease and/or destruction of the lung tissues involved in exchanging oxygen for carbon dioxide (see Box 2-2, “Out With the Old Terms, In With the New”). These problems may be present in different degrees and evolve at different rates. Nevertheless, the changes cause breathlessness (dyspnea), chronic cough, and sputum production. COPD is most often caused by significant exposure to noxious particles and gases, primarily tobacco smoke. The course of COPD may be punctuated by periods of worsening symptoms called exacerbations.
COPD can be prevented, but it cannot be cured. Fortunately, treatment to make breathing easier and prolong life is available for those with the disease.
What Takes Place in COPD?
Inhaling noxious gases or particles causes inflammation in the lungs. When inflammation becomes chronic, changes in lung tissue occur. The airways become narrowed. The bronchi, bronchioles, and alveoli are normally very elastic, which means they stretch and recoil during the process of breathing. In COPD this elasticity is reduced. As a result, the airways and alveoli are no longer able to bounce back to their original shape, especially during exhalation. Some of the airways collapse, preventing some alveoli from deflating and causing air to get trapped in the lungs. This causes parts of the lung to become enlarged, or hyperinflated. Destruction of the alveoli also hampers the exchange of oxygen and carbon dioxide. This leads to too little oxygen and too much carbon dioxide in the blood.
The presence of harmful substances also sparks the increased production of mucus in the bronchial tubes. Under normal circumstances, once the intruder has been eliminated, inflammation and excess mucus production subside. But in people with COPD, the inflammation and excess mucus production persist. In addition, inhaled tobacco smoke damages the hair-like cilia that normally help to sweep mucus out of the lungs and expel toxic substances. Constant inflammation in the airways, an overabundance of mucus, and decreased ability to clear the mucus cause the passageways in the bronchi to narrow. This can cause difficulty breathing and, typically, a chronic cough.
What Causes COPD?
The primary cause of COPD is smoking, but long-term exposure to air pollution, dust, or certain chemicals also may cause or contribute to it.
A diet that is rich in fiber (from whole grains, whole fruits, vegetables, beans, brown rice, and nuts), and low in red meat, refined grains, and sugar may help keep the lungs healthy and reduce the chances of getting COPD for both smokers and nonsmokers. However, it is unknown whether changing fiber intake improves lung function in patients who already have COPD.
Smoking
COPD most often affects people age 40 and older who have smoked a pack of cigarettes per day for 10 or more years. Pipe and cigar smoking also can decrease lung function and increase the chance of COPD, even in people who have never smoked cigarettes. So can smoking water pipes or marijuana.
Smokers who have a family history of COPD are at particularly high risk. For some people, exposure to secondhand smoke can cause respiratory symptoms and possibly COPD. Exposure to secondhand smoke in childhood appears to increase the risk for developing COPD in adulthood. In a 2016 study, middle-aged people whose mothers were heavy smokers (more than 20 cigarettes a day) were more than twice as likely to have lung impairment indicative of COPD than people whose mothers had not smoked.
People who have quit smoking are still at increased risk of eventually being diagnosed with COPD. But stopping smoking significantly reduces the chances of getting COPD, as well as other lung and heart diseases. Smokers with COPD who stop smoking slow the progression of their COPD. Smoking also increases the risk for lung cancer, but this risk declines when a person stops smoking, and continues to decline the longer they go without smoking.
E-cigarettes were introduced into the United States in 2006 as a supposedly safe alternative to tobacco cigarettes. However, it remains uncertain whether they actually are safe. Despite the lack of long-term research, some studies suggest these products may not be as benign as they seem. E-cigarettes typically contain nicotine, a flavoring, and a solvent. According to one study, they also contain additives with unknown health risks (see Box 2-3, “Want a Puff of Insecticide?”).
More studies are underway to assess whether e-cigarettes and other electronic nicotine delivery systems (ENDS) help with smoking cessation. To date, the results of randomized, controlled clinical trials is mixed. As far as safety goes, studies have linked the use of ENDS to changes in airflow that precede COPD, daytime cough, phlegm production, headache, dry mouth, vertigo, and nausea.
In 2016, the Food and Drug Administration began regulating the manufacture, packaging, labeling, advertising, sale, and distribution of ENDS. All ENDS products must carry a warning that the product contains nicotine, and that nicotine is addictive. They are not required to say what other chemicals they contain.
Genetics
Since not all smokers develop COPD, experts believe that a combination of smoking and genetic factors may be at work in those who do get the disease. With the exception of the alpha-1 antitrypsin gene, the specific genes that may be involved are not known, but researchers have begun to identify possible candidates.
Occupational Exposures
Long-term exposure to various kinds of chemicals, fumes, and dust can also harm the lungs and cause COPD.
Several occupations potentially expose workers to inhalants that, when breathed in over long periods of time, can damage the lungs. For example, agricultural workers may be exposed to gases and organic dusts generated by cotton, flax, hay, and grains, or fertilizers and pesticides. Cotton textile workers may inhale cotton dust. Flourmill workers and bakers may breathe in flour and other grain particles. Exposure to coal mine dust over a full working lifetime, even at the federally mandated limits imposed in 1972, produces a cumulative exposure that appears to increase the risk for COPD.
Occupational exposure to chemicals, fumes, and dust can also lead to asthma. It is often very difficult to distinguish occupational asthma from occupation-induced COPD. The primary treatment for either condition, however, is removal of the offending exposure. Similar medications are used to treat both conditions.
Air Pollution
Whether outdoor air pollution from sources such as automobile, factory, and power plant emissions can cause COPD is uncertain. But there is some evidence that it damages the lungs. One study found that people who lived near major roadways (less than 109 yards away) and were exposed over a long period of time to the tiny particles in automobile exhaust had poorer lung function and a faster decline in lung function over time than people living more than one-quarter mile away from a major road.
Another type of outdoor air pollution is ozone. In the upper atmosphere, ozone protects against harmful ultraviolet radiation. When present at ground level, ozone (which forms when exhaust from tailpipes, coal-fired power plants, and other sources mixes with oxygen) is a pollutant. One study found that increased levels of ground-level ozone correlated with increased risk of dying from respiratory illnesses, including COPD. For people who already have COPD, exposure to high levels of outdoor air pollution can exacerbate their condition.
Indoor air pollution from heating and cooking stoves used in poorly ventilated dwellings is a primary cause of COPD for women who live in developing countries. In the U.S. and other developed countries, studies have found that exposure to wood smoke may increase risk for smokers. One study found that smokers who are consistently exposed to both wood smoke (from a fireplace, wood-burning stove, or in the air) and tobacco smoke are at greater risk for COPD than people exposed to just one of these types of smoke. In addition, people who already have COPD and are exposed to both types of smoke experience more frequent and severe symptoms.
Alpha-1 Antitrypsin Deficiency
In a small number of people, COPD is caused by a hereditary disorder called alpha-1 antitrypsin deficiency. Alpha-1 antitrypsin is a protein that prevents an enzyme called neutrophil elastase from damaging the alveoli. People with alpha-1 antitrypsin deficiency lack this protein, and about 75 percent of adults with this deficiency develop COPD. This genetic disorder is most commonly seen in individuals of Northern European ancestry. People with this deficiency who smoke are at particularly high risk of developing severe lung disease, often at a relatively young age.
Symptoms of COPD
COPD often develops gradually over time, making it difficult to diagnose until it is quite advanced. The lungs, with over 300 million alveoli, have an amazing capacity. Not all of these alveoli are used for the day-to-day work of normal breathing. As we age, we lose some of this excess capacity, but in the absence of a lung disease, the lungs continue to function very well.
Because most people never use their full lung capacity, diminished lung function often is not noticed in the early stages of COPD. As the disease gets worse, people may become less active without realizing their lung function is compromised. They may be unaware of the extent of their limitations, and also unaware that these limitations are due to a lung disease. At some point—often at relatively low levels of exertion—the body is no longer able to compensate, and symptoms become impossible to ignore.
The salient symptoms of COPD include:
- Progressive shortness of breath, particularly with exertion (walking, climbing stairs)
- A cough that doesn’t go away
- Sputum (mucus) production, especially in the morning
- Wheezing (a whistling or squeaky sound when you breathe)
- Chest tightness
- In severe disease, fatigue, weight loss, anorexia, fainting during coughing spelling, ankle swelling, depression, anxiety
Shortness of breath is the symptom that drives most people with undiagnosed COPD to see a doctor. At first, shortness of breath is only noticeable with exertion, but eventually breathlessness hampers routine daily activities such as washing, dressing, and cooking. Chronic cough may at first be intermittent, but later may occur every day. For people with COPD, it is common to cough up small quantities of sputum. As the disease gets worse, the sputum may become thicker. Wheezing and chest tightness may or may not be present every day, but often become prominent when people with COPD catch a cold.
The frequency and severity of episodes of coughing and shortness of breath increase as the disease worsens. Fatigue and weakness are common complaints. Weight loss may occur in the more advanced stages of the disease, along with morning headaches due to a build-up of carbon dioxide in the blood overnight.
Having a chronic cough and coughing up sputum when there is no identifiable reason, such as a cold or flu, is not normal. It is important to see a doctor during the early signs of lung disease, because effective treatments are available to assist with breathing and improve quality of life. In addition, smokers who learn they have developed lung disease early in the course of the disease may be able to stop smoking before the disease becomes more serious. Many people with COPD wait until breathing has become a chore and their quality of life is seriously compromised before they consult a doctor. While smoking cessation is still important at that point, it is less effective in preventing serious complications of COPD.
Studies have shown that many current and former smokers display symptoms of COPD even though their lung function tests do not meet the criteria to be diagnosed with the disease. It is still unclear whether their lung function will eventually worsen to the point where they are diagnosed, or whether they should receive treatment.
Exacerbations
Exacerbations are sudden flare-ups of COPD symptoms beyond normal day-to-day variations. Common features include increased breathlessness along with wheezing, chest tightness, increased cough and sputum, change of the color of sputum, and fever. Serious exacerbations may require hospitalization. Studies have found that exacerbations of COPD may speed up loss of lung function, especially for people with mild COPD (see Box 2-4, “COPD Flare-Ups May Worsen Lung Function,” on page 14).

Where you live may make a difference in how often you have an exacerbation. One study found that people with COPD who live in communities that ban smoking in public places were 22 percent less likely to be hospitalized for COPD exacerbations than those living in communities that do not have such laws.
In 30 percent of exacerbations, no cause is identified but a recent retrospective study suggests that blood clots in the lungs (pulmonary emboli, or PE) may be responsible in some cases (see Box 2-5, “The Role of PE in COPD Exacerbations”).
Distinguishing COPD From Asthma
The symptoms of COPD and asthma can be similar, especially in the early stages of COPD, and the two conditions can coexist. Therefore, for some people, especially those who smoke, it may be difficult to make an accurate diagnosis. However, there are some distinguishing characteristics. For example, asthma can affect people at any age, while COPD rarely occurs before age 40. Other key differences between COPD and asthma are listed in Box 2-6, “Differences Between COPD and Asthma.”
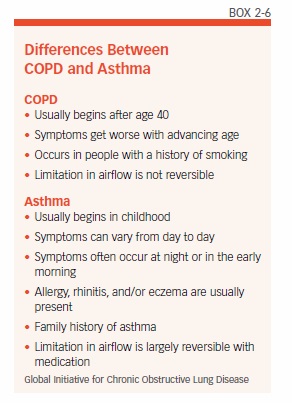
One major difference between asthma and COPD relates to the reversibility of the condition. In COPD, the damage to the airways is not fully reversible. Rather, it is permanent, and gets progressively worse. The airway narrowing in asthma, on the other hand, is usually reversible. In addition, an asthma attack is generally sparked by a trigger, such as an allergic reaction, exposure to the cold, or exercise. Doctors can simulate an asthma trigger with an inhaled drug called methacholine. This drug causes the airways to spasm, which will be detected on a test of breathing function (spirometry, see Chapter 3). A positive result of this test indicates asthma is probably the cause of the person’s symptoms. However, this is not 100 percent accurate because a person with chronic bronchitis also may have a positive result on this test.
People with asthma (especially those who smoke) can develop a chronic cough, and can develop COPD. It may not always be possible to make a clear distinction between asthma and COPD. People suspected of having both COPD and asthma will likely need to see a specialist to confirm the diagnosis. Treatment can be challenging because the two conditions are generally treated differently. Each patient is different—therefore, treatment should be individualized.
COPD and Other Health Conditions
COPD may be a lung disease, but most people with COPD also have other significant chronic diseases. These commonly include skeletal muscle disease, cardiovascular disease, metabolic syndrome, osteoporosis, depress, anxiety and lung cancer. According to the Global Initiative for Chronic Obstructive Lung Disease, the existence of COPD may actually increase the risk for other diseases, lung cancer in particular.
Very severe COPD may cause a type of high blood pressure in the lungs called pulmonary hypertension. Because the lungs are not working efficiently, the heart must work harder to pump blood into the lungs. This can cause high blood pressure in the arteries that bring blood into the lungs. Severe COPD also appears to increase the risk for heart attack, stroke, and heart failure. Heart function may be diminished in patients with COPD, even if they have only mild symptoms. Recently, COPD was found to be associated with peripheral arterial disease (PAD), a form of cardiovascular disease in the legs (see Box 2-7, “PAD More Prevalent in People with COPD”).
Older adults with COPD appear to have an increased risk for a type of mental decline called mild cognitive impairment. They are also more likely to be diagnosed with depression than healthy individuals or those with a different chronic illness (diabetes, for example).
People with COPD are at increased risk for developing shingles, most likely because having COPD weakens the immune system. Shingles is a reactivation of the chicken pox virus that produces a painful rash and can result in lasting nerve damage.
People with COPD are also more likely to catch a cold or the flu, and are more susceptible to getting pneumonia.
The post 2. Chronic Obstructive Pulmonary Disease (COPD) appeared first on University Health News.
Read Original Article: 2. Chronic Obstructive Pulmonary Disease (COPD) »
Powered by WPeMatico