8. Special Health Concerns
Live Better
Although some people use exercise to help reduce risk of disease, it also can be an important way to help you manage a chronic disease, including preserving your independence and ability to do other activities you enjoy. Although starting a new physical activity regimen may be intimidating at first, over time you may find that a particular form of exercise energizes you and lifts your spirits. In some cases you may be able to find groups of people who have the same health condition who you can exercise with, such as a tai chi class for people with heart failure or a water aerobics class for people with arthritis, which can give you some inspiring camaraderie.
Although there are many health issues and conditions that can impact exercise performance and influence the best program for you, this chapter addresses some of the most common concerns, including obesity, cardiovascular disease, diabetes, osteoporosis, frailty, and respiratory issues, including asthma and emphysema. Even if chronic disease makes physical activity more challenging on some days, generally doing something is better than nothing. So do what you can. On days when you’re feeling better, take advantage of it and do more.
Obesity
As introduced in Chapter 2, obesity is defined as a body mass index (BMI) of 30 or more. According to the Centers for Disease Control and Prevention (CDC), obesity affects about 35 percent of U.S. adults. In recent years there has been a significant increase in obesity prevalence among women ages 60 and older, from 31.5 percent a decade ago to more than 38 percent now, averaged across all races. In comparison, about 32 percent of men ages 60 and older are obese. Looking only at black adults in the United States, 39 percent of men and nearly 55 percent of women ages 60 and older are obese. Among Hispanics in the United States, 37 percent of men and 47 percent of women ages 60 and older are obese.
In many cases, obesity is intertwined with other health concerns, such as cardiovascular disease and type 2 diabetes, both of which could be significantly improved by physical activity, and which are addressed in the following sections. Obesity also adds stress to joints and increases risk of arthritis (osteoarthritis). To reduce joint pain in exercise, it may be helpful to use exercise machines that allow you to use your arms and legs at the same time, evenly distributing the load on your joints. Examples include an elliptical cross-trainer machine or Schwinn AirDyne stationary bike. Some people with osteoarthritis find that they perform better in the morning. A physical therapist can provide further guidance on ways to manage arthritis pain during exercise.
If you are obese without other limiting disease conditions and your doctor has cleared you for exercise, standard exercise routines may be appropriate, although if it’s been a long time since you’ve exercised, you will need to ease into it gradually. Aerobic activity is more likely to help you decrease body fat, including harmful abdominal fat, while resistance training can help you retain lean body mass, even when you’re cutting calories. The Physical Activity Guidelines for Americans advise that obese individuals should work toward accumulating at least 300 minutes per week of moderate-intensity aerobic activity to help meet their weight goals. In some cases, two or more shorter sessions a day may be better tolerated and can help you reach this goal more easily.
Cardiovascular Disease
Cardiovascular disease (CVD) is a broad term that encompasses atherosclerosis, heart failure, stroke, heart attack, hypertension, and peripheral arterial disease (difficulty getting blood to your legs and arms). Having one of these conditions doesn’t necessarily mean you can’t exercise. In fact, appropriate exercise training generally can help improve such conditions. Exercise can help control weight and improve blood pressure and blood lipids (triglycerides and cholesterol), which can improve cardiovascular disease risk factors. Regular physical activity also may reduce the need for medications. Importantly, exercise also has been shown to improve quality of life in CVD and make it easier to perform basic self-care tasks.
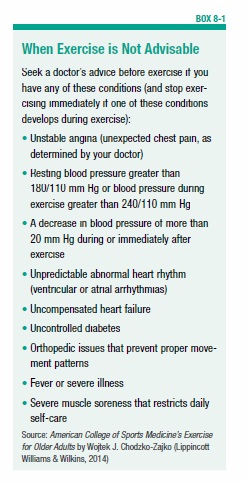
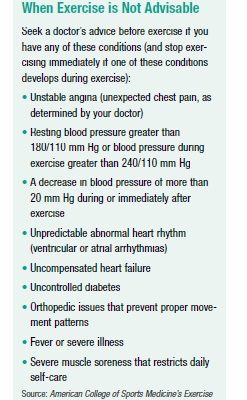
Even so, there are certain precautions a person with CVD should take. In high-risk CVD, exercise may not be recommended (see Box 8-1, “When Exercise is Not Advisable”). In some cases, those with higher risk CVD status may need to exercise under supervision by trained health personnel, such as at a cardiac rehabilitation center. Other people with CVD may be able to exercise on their own after seeking their doctor’s guidance. Both aerobic and resistance training are generally recommended for people with CVD who have their doctor’s approval to exercise. A cool-down session immediately after exercise is especially important for people with CVD since most problems associated with exercise in CVD occur after exercise.
CVD medications also must be considered and discussed with your doctor before starting exercise. For example, medications that dilate (widen) arteries, such as the vasodilator hydralazine, may trigger lightheadedness due to blood pressure lowering. People taking such medications may find warming up before exercise and increasing exertion gradually especially helpful. Also, if you’re taking medications called beta blockers, which may be prescribed after a heart attack or to treat abnormal heart rhythms (arrhythmias), it’s important to realize that these drugs lower your heart rate. So, that can impact your target heart rate for exercise, as well (discussed in Chapter 2 on page 18). Your doctor can help determine the appropriate target heart rate for you using a short exercise stress test. Alternately, you can keep your exercise intensity in check by exercising hard but not to the point where it’s difficult to talk.
Diabetes
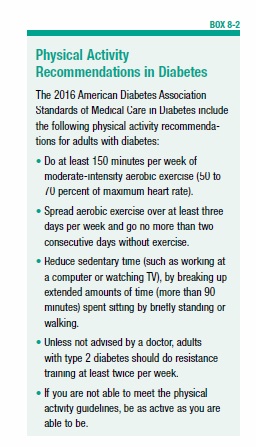
If you have type 2 diabetes or prediabetes, important reasons to exercise include its ability to help improve blood sugar control, enhance insulin sensitivity (which makes your body’s cells more responsive to insulin), and reduce cardiovascular disease risk factors. General physical activity recommendations in diabetes are described in Box 8-2, with more specific recommendations covered in the following pages.
In the short-term, exercise can help lower blood sugar by using glucose to fuel working muscles. In fact, in sustained moderate exercise sessions, muscles take up glucose at almost 20 times the normal rate. Additionally, exercising muscle can absorb glucose on its own, without the use of insulin, and muscle cells also become more responsive to the effects of insulin with exercise. In fact, a single exercise session may increase insulin sensitivity for up to two or three days (and you should exercise regularly to maintain this effect). So, you’ll need less insulin to do the same job and you’ll reduce surges in insulin that can contribute to heart disease, high blood pressure, and other health concerns.
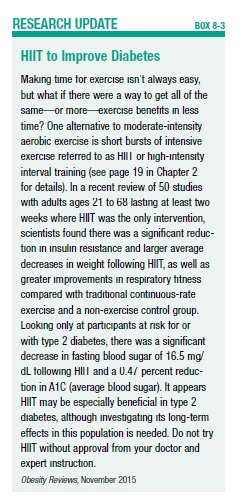
Keeping up an exercise regimen over the long-term can help with weight control and maintaining muscle mass, too. Resistance exercise in combination with aerobic exercise may be especially helpful in improving A1C (average blood sugar) in type 2 diabetes. In some cases of regular exercise, your doctor may even be able to reduce your diabetes medication. New research suggests high-intensity interval training (HIIT) may be another exercise option in type 2 diabetes management or prevention (see Box 8-3, “HIIT to Improve Diabetes,” on page 77).
Although the role of exercise in controlling blood sugar is not as clear in type 1 diabetes, the American Diabetes Association considers exercise just as important in type 1 diabetes as it is for the general population. Studies suggest many benefits of regular exercise in type 1 diabetes, such as improved cardiovascular health and improved insulin sensitivity, as well as reduced risk of long-term complications. However, as discussed in the next section, people with type 1 diabetes (and those taking certain diabetes medications) must follow special precautions to guard against low blood sugar during exercise.
Exercise and Blood Sugar
Special precautions must be followed to ensure your blood sugar is in reasonable control before engaging in exercise, especially if you have type 1 diabetes. Exercise performance seems to be best when blood sugar is maintained between 80 and 180 mg/dL. Generally, experts don’t recommend starting an exercise session if your blood sugar is higher than 250 mg/dL and ketones are present (which can be checked with urine test strips sold at pharmacies). Ketones are a chemical compound produced when a person with diabetes doesn’t have enough insulin available to use glucose for energy.
Also note that short sessions of high-intensity activity may make your blood sugar go up (regardless of which type of diabetes you have), due to the body’s release of certain hormones that raise glucose to help fuel physical activity. This is usually temporary, and within a few hours after intense exercise your blood sugar will come back down as glucose is used to replenish glycogen (glucose stores) in your muscles. You typically shouldn’t increase (but rather, will likely need to decrease) your post-workout insulin dose in this situation. If you don’t take insulin, just realize it may take a little time for your blood sugar to come down after intense exercise, or you can cool down with some less intense exercise to help bring your blood sugar back to normal.
Another concern if you are taking insulin or sulfonylurea medications (such as glyburide and glipizide, which stimulate insulin release), is that you may experience hypoglycemia (low blood sugar) during exercise if adjustments aren’t made (see Box 8-4, “Tips to Addressing Exercise and Blood Sugar,” on page 78).
Exercise and Diabetes Complications
The longer you have had diabetes, the more likely you have developed microvascular complications (diseases of the smallest blood vessels) related to diabetes that could impact your exercise program, requiring certain precautions during exercise and/or requiring the avoidance of certain kinds of physical activity. Such conditions include retinopathy (eye disease), peripheral neuropathy (nerve disease), and nephropathy (kidney disease). Your healthcare team can assess your condition and determine what types of exercise are appropriate and whether any restrictions are needed. Following are some general guidelines from the American Diabetes Association (ADA).
Retinopathy
With appropriate precautions, people with diabetic retinopathy can often do both aerobic and resistance exercise.
➧ Good activities: Moderate-intensity and low impact exercises, such as walking, water exercise, and bicycling. With appropriate instruction, tai chi and yoga can be good options, too.
➧ Risky activities: Strenuous exercise or physical activity that requires heavy lifting and straining, holding your breath while lifting or pushing, isometric exercise (a type of strength training), and high-impact activities that require jarring, head-down positions, or positioning your arms over your head.
If you have proliferative diabetic retinopathy (a rapidly increasing number of fragile blood vessels in the eye) or severe nonproliferative diabetic retinopathy, your ophthalmologist will likely advise you to avoid vigorous-intensity aerobic activity, and possibly resistance exercise, too.
Peripheral Neuropathy
Peripheral neuropathy can cause weakness, numbness, and pain, particularly in the hands and feet. It can result in decreased sensation of pain in your hands and feet, which can increase risk of injury to your skin and infection.
➧ Good activities: Moderate weight-bearing activities that are low-impact, such as walking, bicycling, swimming, and chair exercises. Exercise in a moderate climate.
➧ Risky activities: High-impact, strenuous, or prolonged weight-bearing activities, such as walking a long distance, running on a treadmill, jumping/hopping, exercise in heat or cold, and weight-bearing exercise when you have a foot injury, open sore, or ulcer.
➧ Precautions to take: Wear proper shoes to protect your feet and check your feet every day to detect any wounds early. The ADA recommends shoes with silica gel or air mid-soles because they help reduce stress on your feet and joints. The ADA also recommends socks made of material that helps pull moisture aware from your skin, such as CoolMax, polypropylene, or acrylic. Always check your feet before and after activity for blisters, redness, or irritation. If you have a foot injury or open sore, only do non-weight-bearing activities (such as riding a stationary bike or swimming).
Autonomic Neuropathy
Autonomic neuropathy is another type of nerve damage and affects the nerves in your body that control your body systems, such as the heart and blood vessels, sweat glands, and eyes. If you have this condition, talk to your doctor before starting an exercise program because you may need an exercise stress test first.
➧ Good activities: Mild to moderate aerobic activities and resistance training, but increase the length of time you exercise slowly and follow your doctor’s recommendations.
➧ Risky activities: Exercising in extreme heat in which dehydration can occur, and activities that require rapid changes in movement that could cause you to faint.
Nephropathy
In diabetic nephropathy, physical activity can temporarily increase loss of protein in the urine. However, there is no evidence that vigorous-intensity exercise increases the rate at which diabetic kidney disease progresses, and no specific exercise restrictions may be needed.
➧ Good activities: Light to moderate daily activities such as walking, light household chores, gardening, and water exercise.
➧ Risky activities: Strenuous activity. Follow your doctor’s advice.
Osteoporosis
In its early stages, osteoporosis is a silent condition in which bones become thinner and more brittle over time. As you reach your 60s and 70s, you may start to show outward signs of osteoporosis, such as breaking fragile bones from a minor fall (most commonly the hip, spine, or wrist). As the bones in your spine lose mineral density, kyphosis can appear, which causes hunching or rounding of your spine and also may cause pain. Osteoporosis affects both men and women, but it typically affects women at a younger age, due in large part to the significant loss of bone mass (up to 20 percent) in the five to seven years after menopause. Osteoporosis tends to affect men around age 70 and older. Risk of osteoporosis also increases with factors such as smoking, high alcohol intake (three or more drinks per day), family history of osteoporosis, limited physical activity, and certain drugs that cause bone loss (see Box 8-5, “Medicines and Bone Loss”).
Exercise and Bone Health
You can fight back against osteoporosis with good nutrition (see the section on “Structural Nutrients” in Chapter 3, page 32) and physical activity, and in some cases you may need to take bone-strengthening medications. In general, resistance training (two or three sessions per week), and weight-bearing aerobic activity (at least four sessions per week) are recommended to assist in maintaining and preventing bone loss. Remember, people reach peak bone mass around age 30, so your goal after that point is to hold on to as much bone mass as you can, minimizing loss as you age.
Resistance exercise causes muscle to contract against bone, and this stimulates the bone to become stronger and denser. As mentioned in Chapter 2, resistance (strength) training is especially important for strong bones. In 1994, Miriam Nelson, PhD, and her colleagues at Tufts University published a ground- breaking study showing that postmenopausal women (ages 50 to 70) who lifted weights twice a week for a year gained an average of 1 percent of their bone mass, while those who didn’t exercise lost about 2 percent of their bone density, which is typical after menopause. Since then, other studies have confirmed that strength training can support bone health. Recently, preliminary results from an ongoing study were released suggesting that heavy-load resistance training not only may be more beneficial for bones in postmenopausal women but also safe (see Box 8-6, “Heavy Lifting for Bones”).
Weight-bearing aerobic exercise can support bone health, too, although high-impact activity such as running or jumping rope may help improve bone more quickly compared to low-impact activity, such as pounding your feet against the pavement in a brisk walk, which could take years to show a significant change in bone health (despite its more immediate cardiovascular benefits). High-impact aerobic activity isn’t safe for everyone, though, so check with your healthcare team first. As for non-impact aerobic exercise, such as swimming, water aerobics, and bicycling, it does not seem to place a sufficient load on the bone tissue to maintain or improve bone density, although you may still do such exercise to support cardiovascular health.
Proceed with Caution
If you have osteoporosis, seek your healthcare team’s guidance, including consulting a physical therapist experienced in osteoporosis, and discuss the best exercise program for you. They may use tests such as the 30 Second Sit-to-Stand Test (shown in Box 2-9 on page 22), to assess weakness and risk of falling. If you’re unable to do at least eight chair stands in 30 seconds, you may be at increased risk of falls. A physical therapist also can assess kyphosis (an overly rounded back) and determine if there are exercises you should avoid. Expert instruction in correct technique for resistance training is especially important for those with poor bone health.
Frailty
Although people of any age can have frail health, it’s more common in those over age 65. Approximately seven percent of people over age 65 would be considered frail based on having at least three of the following five criteria at the same time:
- Poor muscle strength
- Physical exhaustion
- Low physical activity (sedentary)
- Slow walking speed
- Unintentional weight loss
Those who have one or two of the above criteria may be considered to have prefrailty. For example, if you find that simple things are getting difficult, such as getting up out of your easy chair, your appetite is lagging, and you’re getting too thin, you could be on the path to frailty. Exercise may help you fight back against frailty, even if you’re well into your golden years and have never been very physically active (see Box 8-7, “Physical Activity for Fighting Frailty”). That’s important, because if you can put the brakes on frailty, you may be able to reduce your risk of becoming disabled or losing your independence.
The three main goals of physical activity in frailty are to increase your muscle strength, increase cardiovascular endurance, and increase your overall level of physical activity. How you get there should be based on your individual ability and needs, and it is generally best directed by an exercise professional, such as a physical therapist, who is well-versed in working with those who are frail and can provide appropriate exercise testing prior to beginning a program. Your healthcare team also will need to consider medications you’re taking, which may impact your risk for falls, dizziness, fatigue, and other side effects.
Once frail individuals increase their activity, appetite often improves, but if it doesn’t, you may need to consult with a registered dietitian nutritionist who can help you with strategies for stimulating your appetite and maintaining your weight. A focus on eating a greater amount of healthy, nutrient-dense foods is generally needed, as discussed in Box 8-8, “Increasing Calories and Nutrition.”
Asthma and COPD
Asthma is relatively common in older adults and can make it more difficult to breathe during and, more commonly, after exercise. If you are prone to exercise-induced asthma, you should always carry your inhaler with you. An easy, slow warm-up may help reduce the risk of an asthma attack. For example, you might do light aerobic exercise (such as walking) below 50 percent of your target heart rate for five to 10 minutes to warm up. If you have just gotten over a cold or flu, you will be even more at risk for breathing problems during exercise, so start back slowly in your exercise regimen, exercising less intensely and for a shorter time period at first.
COPD or chronic obstructive pulmonary disease is another condition that can impact breathing and most commonly includes bronchitis (inflammation of the bronchial tubes, which carry air to the lungs) and emphysema (destruction and enlargement of air sacs in the lungs, which is most commonly caused by smoking). Exercise is considered an essential component of treating COPD, because it can help your body learn to better use oxygen and help build your energy levels and tolerance for physical activity. It’s generally best to do exercise that has a relatively consistent intensity, such as walking and stationary cycling, rather than varying intensity, such as dancing and tennis. Low-intensity strength training is also relatively safe for people with COPD. As with asthma, the warm-up and cool-down are especially important for people with COPD, giving the lungs time to slowly adjust.
The post 8. Special Health Concerns appeared first on University Health News.
Read Original Article: 8. Special Health Concerns »
Powered by WPeMatico